The Real Cost of Addiction
Treating Methamphetamine Addiction
- The most effective treatments for methamphetamine addiction so far are behavioral therapies, such as cognitive-behavioral therapy, which helps patients recognize, avoid, and cope with the situations in which they are most likely to use drugs combined with motivational incentives, which uses vouchers or small cash rewards to encourage patients to remain drug-free.
- The matrix model is most commonly recommended model for treating methamphetamine.
- Special considerations for treatment of methamphetamine addiction:
-
- Rest Period: During the acute withdrawal phase (approx. 7-10 days), it may be best to let the individual rest if they want to sleep without engaging in therapy.
- Harm Reduction: Risky sexual behavior is common among methamphetamine users due to increased sex drive and increased risk taking propensity. Condom promotion programs, safer sex education and safer sex negotiation for both male and female methamphetamine users, and HIV/AIDS testing can reduce these risks.
- Sexual Issues: A common concern of persons who use methamphetamine is reduced sexual drive and should be addressed during therapy.
- Exercise may enhance the effectiveness of treatment for individuals with methamphetamine use disorder.
- Harm reduction efforts should be incorporated to address high risk sexual behavior.
Predicting and Preventing Relapse
It is important to engage methamphetamine users in abstinence-promoting resources and enhanced continuing care post-treatment because the majority of relapses occur within 6-12 months following treatment.
-
- Risk of relapse remained years after treatment discharge with 25% relapse in years 2-5 post treatment, pointing to a need for continuing availability of resources to the long-time abstinent methamphetamine user.
Protective factors predicting longer time to relapse following methamphetamine treatment included:
-
- Having experienced serious problems perceived as related to methamphetamine use
- Longer treatment episode
- Participation in self-help and/or additional SUD treatment during the abstinence period (strongest effect size)
Current treatment protocols and recommended approaches
If you have private insurance, contact the customer services/behavioral health number on the back of your card. You may also have an EAP (Employee Assistance Program) through your employer who can assist you. If it is an emergency, please go to the nearest Emergency Department.
- Meth’s Resurgence Spotlights Lack Of Meds To Combat The Addiction, Kaiser Health News, 2019
This article provides a nice summary of the current situation with methamphetamine and the challenges for treatment, as well as a brief blurb about how to approach this addiction with the existing limitations. It also includes information about efforts to develop drugs to combat meth addiction.
According to National Institute on Drug Abuse the most effective treatments for methamphetamine addiction so far are behavioral therapies, such as: Drug Facts
-
- Cognitive-behavioral therapy, which helps patients recognize, avoid, and cope with the situations in which they are most likely to use drugs
- Motivational incentives, which uses vouchers or small cash rewards to encourage patients to remain drug-free
While research is underway, there are currently no government-approved medications to treat methamphetamine addiction. However, there are medications which may help to manage some of the symptoms that occur during the withdrawal process. americanaddictioncenters.org/meth-treatment/withdrawal
- Matrix Model, Current Research On The Epidemiology, Medical And Psychiatric Effects, And Treatment Of Methamphetamine Use, 2014
Richard Rwason, PhD, one of the developers of the Matrix Model states, “To date, there is limited literature on evidence-based pharmacological treatment approaches for methamphetamine withdrawal. Antidepressants and anxiolytics may be used to ameliorate depressive and anxiety symptoms, though research suggests only limited benefits of antidepressants in reducing withdrawal symptoms.”
“We have data from treating several thousand patients [with the Matrix model],” Rawson said. “Treatment of meth addiction appears approximately equal to cocaine treatment. Treatment is about 50 percent to 60 percent drug-free at the end of one year.” That’s superior to recovery after behavioral therapy for heroin addiction (without the use of methadone), but not as good as recovery from alcoholism, according to Rawson. No nationwide statistics on the overall effectiveness of treatment for meth addiction exist, but as the Matrix model is a particularly vigorous, well-studied approach, it’s likely this success rate is higher than average, Rawson noted.
Treatment Improvement Protocol (TIP) Series, No. 33, SAMHSA/Center for Substance Abuse Treatment.
ncbi.nlm.nih.gov/books/NBK64329
This is the primary guidance document available from SAMHSA which provides generalized treatment considerations and guidance for all stimulants including amphetamines. Does not provide specific guidance for methamphetamine but does note differences specific to methamphetamine throughout.
Resource #4, provides a very informative article summarizing one treatment center’s process of applying this protocol to treating methamphetamine including practical considerations, lessons learned and procedural changes established (refer to resource #4)
Chapter 2, Methamphetamine, describes how methamphetamine affects the brain and compares to the effects of other stimulants.
Methamphetamine Specific Considerations Noted:
Rest Period Before Therapy:
- According to TIP 33, The initial period of stimulant abstinence is characterized by symptoms of depression, difficulty concentrating, poor memory, fatigue, craving, and paranoia. The duration of these symptoms varies; however,they typically last 10 to 15 days for methamphetamine users (TIP 33, chapter 4).
- During the acute withdrawal phase (approx. 7-10 days), it may be best to let the individual sleep if they want to sleep without engaging in therapy. Research documents that during this acute phase, there is increased sleeping and eating, depression-related symptoms and, less severely, anxiety and craving-related symptoms. Oversleeping was marked during the acute phase and despite a reduction in sleep quality, was not followed by a period of insomnia during the subacute phase. The nature, time course and severity of methamphetamine withdrawal, 2005.
- Prairie Ridge addiction treatment center noted that patients are tired for 10-15 days of withdrawal, don’t make them go to therapy sessions during that time if they want to rest. If they are incarcerated, this rest period can be done in jail. One Program’s Transition to Research-Based Strategies for Treating Methamphetamine Abuse, 2007
- Sexual Issues: According to TIP 33, Chapter 4, stimulant-dependent clients can have tremendous concerns and anxieties about the compulsive sexual behaviors they engage in while using stimulants. Client fears should be addressed, such as the fear that sex without drugs will be boring or impossible.
- Urinalysis Screens: According to Tip 33, Chapter 4, stimulant-dependent clients in outpatient programs need structure that provides support for engaging in healthy behaviors. Urine testing is part of that structure. It should not be presented or used primarily as an investigative tool or to test the honesty of clients. Rather, it should be used and presented as a means of support for initiating and maintaining sobriety.
- A research study assessing the process of care measures found that sustained abstinence from methamphetamine during outpatient treatment was a strong predictor of testing negative for methamphetamine at both 12-month and 36-month follow-ups. Researchers concluded that monitoring drug use during treatment may improve client abstinence during treatment.
- Process-of-care measures as predictors of client outcome among a methamphetamine-dependent sample at 12-and 36-month follow-ups. J Psychoactive Drugs. 2012 Sep-Oct;44(4):342-9., Rawson RA1, Gonzales R, Greenwell L, Chalk M.
- One Program’s Transition to Research-Based Strategies for Treating Methamphetamine Abuse, 2007
- This article summarizes the process of a treatment center to use the NIATx model to improve treatment outcomes for individuals with methamphetamine use disorder based on guidance provided in TIP 33.
- One Program’s Transition to Research-Based Strategies for Treating Methamphetamine Abuse, 2007
New Practices Adopted Included
Prairie Ridge addiction treatment center offers residential substance abuse treatment for adult men and women. The average length of stay is 28 days, and all residential programs and living arrangements are gender-specific. Detox services are not available on-site.
- Relapse “slips” should be regarded not as failures, but as opportunities to reevaluate the treatment plan.
- Rest Period: Patients are tired for 10-15 days of withdrawal, don’t make them go to therapy sessions during that time if they want to rest. If they are incarcerated, they do this rest period in jail.
- They found that clients do not always need the full 10 to 15 days suggested by the TIP before engaging in treatment; in most cases, a few days of downtime monitored by their residential program nurse was sufficient. The implicit message this new approach sends our clients is not simply that they will benefit from a period of recuperation, but also that we understand their needs and state of mind.
- Increased sexual urges and stress about this topic is addressed. Methamphetamine-abusing clients frequently reported that the drug enhances sex and abstinence spoils it. TIP 33 persuaded us that failing to address sexual feelings and experiences in treatment can compromise some clients’ chances for recovery.
- No longer encourage methamphetamine clients to consider using an antidepressant.
- Did not have enough counselors to form groups of only methamphetamine users so they presented most of the information to methamphetamine-abusing clients during individual counseling sessions, but also use some recommendations in group sessions, such as giving gift coupons to encourage attendance.
- Exercise may improve outcomes: Research indicates that exercise may improve depressive symptoms among individuals in treatment for methamphetamine use disorder
- Finding a “Fix” for Meth Addiction – Can Exercise Help?, 2016
- This article summarizes a study with 135 methamphetamine-dependent people, newly enrolled in residential treatment found that:
-
- Exercise had a significant effect on reducing depression and anxiety (Published in the Journal of Substance Abuse Treatment)
- Exercise participants with the most severe medical, psychiatric, and meth disorders upon entering the study showed the most significant improvement in depressive symptoms by the end of the study – suggesting that exercise is particularly beneficial to such individuals. (Published in the American Journal of Addiction)
- Following treatment in the residential program, participants were interviewed, and urine samples were collected at 1-, 3-, and 6-months. Fewer exercise participants returned to meth use compared to education participants at all three time periods, but differences were not statistically significant. However, lower severity users in the exercise group had a lower percentage of positive urine results and fewer days of meth use in the previous 30 days as measured by self-report, at the three time points than did lower severity users in the education group, leading the authors to conclude that their results support the value of exercise as a treatment component for people using meth 18 or fewer days per month (the cut-off for lower severity use.) (Published in Drug and Alcohol Dependence)
Meth use disorder is associated with brain changes known as striatal dopaminergic deficits that have been linked to poor treatment outcomes. Brain imaging scans after 8 weeks for those in the exercise group showed significant positive brain changes, but those in the education group did not. (Published in Neuropsychopharmacology)
UCLA Integrated Substance Abuse Programs, Methamphetamine Abuse: Long-Term Trajectories, Correlates, Treatment Effects. An 8 year follow up to a study that included 596 people, half recruited from drug treatment participation in Los Angeles County and half with no prior meth treatment at recruitment. This is an ongoing study, but as of 2015 they reported that:
-
- Among those receiving treatment for methamphetamine, 61% relapsed within 1 year after discharge and another 25% relapsed during years 2-5.
- Protective factors predicting longer time to relapse included:
-
-
- having experienced serious meth-related psychiatric/behavioral problems,
- longer treatment duration, and
- participating in self-help or other treatment during the posttreatment abstinence period
-
-
- Risk factors predicting shorter time to relapse included:
-
-
- having a parent with alcohol and/or drug use problems, and
- involvement in meth sales.
-
-
- In-depth qualitative interviews indicate that individualized interventions and multiple, simultaneous approaches and resources were essential in reaching stable abstinence (Herbeck, Brecht et al., 2014).
- Time to relapse following treatment for methamphetamine use: a long-term perspective on patterns and predictors, NCBI, 2014
- Like the previous study, this research assessed time to relapse to identify predictors with a sample of 350 participants over a 5-year period. The study conclusions almost mirror those of the previous article:
- The highest rates of relapse occurred early in the post-treatment period, with half the sample relapsing within six months. This predominant early relapse emphasizes the need for continuing care and strategies for connecting/engaging methamphetamine users to abstinence-promoting resources immediately following SUD treatment (Dennis and Scott, 2012; McKay et al., 2009; Laudet and Humphreys, 2013).
- For more information about effective continuing care methods post-treatment refer to this article
- While the risk of relapse decreased with increasing duration of continuing abstinence, some risk of relapse remained years after treatment discharge, thus pointing to a need for continuing availability of resources to the long-time abstinent methamphetamine user.
- Study results showed potential vulnerabilities that could be easily identified at treatment admission, such that specifically targeted interventions could be strengthened. Results also show that even with such vulnerabilities, longer duration of treatment and continuing treatment and/or self-help are associated with longer duration of continued abstinence for methamphetamine users. Vulnerabilities include:
-
-
- Risk factors predictive of shorter time to relapse included parental drug use and ever having sold methamphetamine
- Protective factors predicting longer time to relapse included:
-
-
-
-
-
- Having experienced three serious problems perceived as related to methamphetamine use (paranoia, hallucinations, violent behavior)
- Longer treatment episode
- Participation in self-help and/or additional SUD treatment during the abstinence period (strongest effect)
-
-
-
- Harm Reduction Treatment Interventions for Rural Methamphetamine Abuse, 2017
- High risk sexual behavior:
- Condom promotion programs as well as safer sex education and safer sex negotiation for both male and female methamphetamine users can be part of harm reduction activities for methamphetamine users.
- Low-cost (possibly free) HIV/AIDS testing and information on how to conduct less risky sexual behaviors.
- Injection Drug Use:
- Needle exchange programs to give individuals an opportunity to practice safer use.
- The availability of smoking equipment such as pipes may reduce injection use.
- Distribution of empty capsules that the consumer can place their dose of methamphetamine in. This is safer than needles but can lead to extensive stomach damage.
- Establishment of harm reduction facilities that are accepting, non-stigmatizing and provide food, and support services could be useful for engaging methamphetamine users into a safe environment.
- Distributing a legally, laboratory-produced prescription stimulant such as Adderall or Ritalin to help users titrate their methamphetamine tolerance at their convenience, with a treatment plan goal of abstinence eventually.
Crystal Meth Withdrawal, americanaddictioncenters.org/meth-treatment/withdrawal
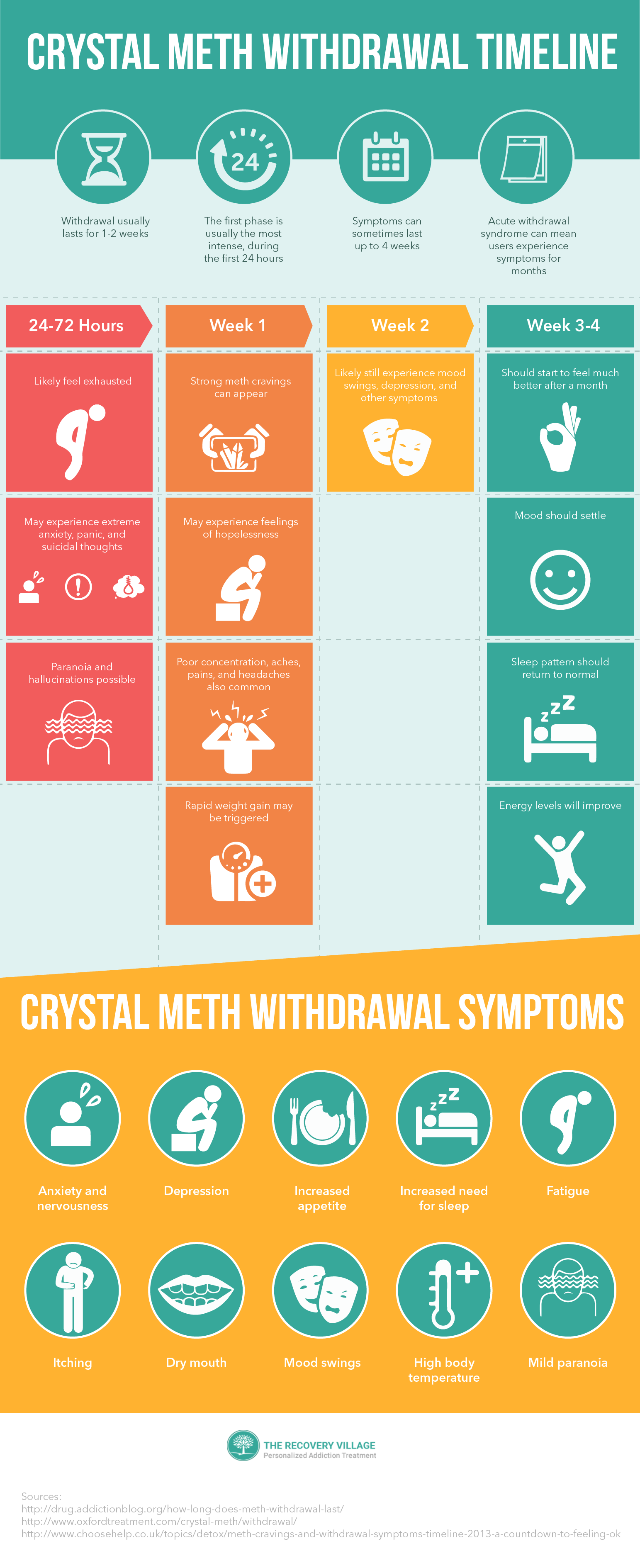
Methamphetamine has a relatively short half-life (an average around 10 hours), and it is a fast-acting drug. In general, according to research, it appears that the timeline for withdrawal from crystal meth is fairly consistent among users:
- It begins within the first 24 hours of abstinence.
- It reaches its peak within the first 7-10 days following discontinuation of the drug, and there is a steady decline in the intensity of symptoms following this peak.
- It has an average duration of about 14-20 days, with 14 days being the most commonly reported duration of the withdrawal syndrome.
According to the same research and several other studies, it appears that the primary symptoms during this withdrawal period consist of:
- Feelings of fatigue, lethargy, and excessive sleepiness (typical of withdrawal from stimulant medications) are common.
- Increased appetite, dry mouth, and some episodes of jitteriness generally occur.
A significant number of individuals report feelings of depression, which were also noted to decline over the course of the withdrawal time period. These depressive symptoms can be significant and associated with thoughts of suicide. In addition, research has indicated that a good number of individuals who relapse do so because of feelings of depression, apathy, hopelessness, etc.
Extreme cravings for methamphetamine also occur during the withdrawal process but decline rapidly. Cravings for methamphetamine during withdrawal appear to be associated with the level of depression occurring in the individual. In addition, as one would expect, research indicates that the more intense and frequent the cravings an individual in withdrawal from methamphetamine experiences, the higher the probability that the individual will relapse during the withdrawal syndrome.
Psychotic symptoms, such as paranoia, hallucinations, and delusions, also occur in many individuals. These symptoms need to be addressed in a professional treatment environment.
A large meta-analysis indicated that the most dangerous symptoms associated with methamphetamine withdrawal are severe depression and the potential to develop psychosis. It did not reveal any significant overall risk for the development of other health issues, although in individual cases, there may be health risks associated with withdrawal from methamphetamine. These risks may be more salient in older individuals or individuals with pre-existing medical conditions.
There are no medications approved by the FDA that are specifically designed to be used in the detox withdrawal process from crystal meth. However, there are several different medications that can help to manage some of the symptoms that occur during this process of withdrawal. Research supporting the efficacy of medications to ease withdrawal symptoms is limited.
In the management of the withdrawal process from crystal meth, physicians are free to use any medications to address any specific symptoms that occur in individuals. For instance, in individuals who develop psychotic-type behaviors, such as paranoia, delusions, and/or hallucinations, physicians are free to administer antipsychotic medications to these individuals if the symptoms are judged to be severe enough to require direct treatment.
Physicians may also attempt to directly manage depressive symptoms with antidepressants; however, because most antidepressants do not begin to exert their effects until 2-4 weeks after initial administration, this may not be an effective means of coping with depression in the withdrawal process.
- Wellbutrin (bupropion): This drug is an antidepressant that has been approved for and used in smoking cessation programs. It also has a good body of research indicating that it is useful in reducing the symptoms of withdrawal in individuals who have abused crystal meth. It appears to reduce the significant cravings associated with the withdrawal process and appears to be more appropriate for light to moderate methamphetamine use disorders.
- Provigil (modafinil): This medication is a mild stimulant medication that is used in the treatment of ADHD and in the treatment of narcolepsy. The mild stimulant properties of the medication can assist in reducing issues of with disruptive sleep patterns and may also help those in recovery with increasing energy and enhancing concentration.
- Selective serotonin reuptake inhibitors: Paxil (paroxetine) is a selective serotonin reuptake inhibitor (a specific type of antidepressant medication) that has been shown in some studies to relieve cravings in abstinent crystal meth users going through withdrawal; however, the research on the efficiency of this drug for treatment during crystal meth withdrawal is mixed. There is research that has suggested that Prozac (fluoxetine) may be useful in the treatment of crystal meth addiction during the withdrawal process.
- Remeron (mirtazapine): Remeron is an atypical antidepressant that has its primary mechanism of action on both serotonin and norepinephrine. There is evidence that its use can help to prevent relapse during the withdrawal process.
{kind=link}
The DSM IV-TR identifies dysphoric mood as the main symptom for amphetamine (including methamphetamine) withdrawal and requires at least two of the following additional symptoms for a positive diagnosis: fatigue, insomnia or hypersomnia, increased appetite, psychomotor agitation or retardation and vivid, unpleasant dreams.
No recommended detox protocol was found however, related findings include:
-
-
- In this study, methamphetamine withdrawal symptoms (aside from craving for methamphetamine) were, on average, mild and resolved within 14 days of abstinence. Cravings lasted at least 5 weeks.
- Severity of methamphetamine withdrawal symptomatology (which varies considerably among methamphetamine-dependent individuals) is likely to influence the ability of methamphetamine-dependent individuals to maintain abstinence.
-
- Treatment for Crystal Meth Withdrawal, American Addiction Centers, 2019
- There are no FDA approved drugs to assist individuals with the detox from Meth, but there are some medications that may help manage some of the symptoms:
-
- *Wellbutrin (antidepressant)
- *Provigil (assists in regulating sleep patterns, concentration)
- *Prozac and Paxil (mixed reviews, might help with cravings)
- *Remeron (antidepressant that may be used to help prevent relapse during withdrawal period)
- *These drugs are not paid for by Medicaid as part of a medication assistance treatment method. Medacaid.gov, 2014
Promising Research!
NIDA research is supporting the development of vaccines for cocaine, opioids, nicotine, and methamphetamine. The vaccines work by stimulating the body’s own immune system to produce antibodies that target and bind the drug’s molecules in the bloodstream and prevent them from reaching the brain. The cocaine and nicotine vaccines have had promising results in human trials, effectively reducing drug use in those patients who are able to achieve high antibody levels as a result of vaccination. More info on the vaccine.